
Right Treatment.
First Time.
Most UTI treatment failure does not begin with the antibiotic. It begins when diagnostics fail to provide accurate direction.
UTI treatment failure is high. The cost is even higher. UTIs disproportionately drive repeat visits, unnecessary antibiotic exposure, avoidable callbacks, and downstream cost across outpatient care. The problem is not a lack of treatment options. It is that conventional testing often does not tell clinicians, quickly and accurately enough, what antibiotic is most likely to work. Pathnostics helps practices move beyond detection alone and toward direction that supports better first-pass decisions.
When the First Answer Is Wrong,
Everyone Pays.
In UTI management, failure is often treated as routine. A patient does not improve, another antibiotic is prescribed, another callback happens, another visit follows, and the system moves on. But the cost is real and largely avoidable.
The first failed answer is not a harmless step in the process. It is often the moment that triggers a cascade of unnecessary cost, work, and patient harm.
For the Patient
More days sick. More antibiotic exposure and collateral impact. More frustration. More risk that recurrence becomes the next normal.
For the Practice
Increased cost and lower efficiency driven by more callbacks, repeat prescriptions, staff burden, and operational drag from an infection that should have been resolved earlier.
For the System
Avoidable waste, cost of escalated care, and increased antibiotic resistance from misinformed first-pass antibiotic decisions.
Today's Testing May Not Adequately Detect
and Does Not Reliably Direct.
The issue is bigger than turnaround time. The conventional model was not built to answer the modern clinical question that matters most: which therapy is most likely to work against the infection as it actually behaves in the patient?
Standard culture misses important infections
Culture was built around outdated assumptions and performs poorly in polymicrobial, fastidious, gram-positive, and other clinically relevant infections.
Traditional AST can fall short on real-world direction
Testing isolated organisms one by one can miss how the total infection behaves when multiple organisms are present together.
PCR with or without extras can misdirect
Detection matters, but detection is not direction. Resistance markers show poor concordance with infection behavior and unproven technologies should not be counted on when an antibiotic prescription is in order.
Clinicians do not just need to know what may be present. They need clinically actionable direction fast enough to make the first treatment decision count.
Detection Is Important.
Direction Is What Changes Outcomes.
The future of UTI diagnostics is not just finding more organisms. It is answering the clinical question that matters most: what is most likely to work for this patient's infection as it exists in the real world. That requires moving beyond methods that infer response from isolated organisms or molecular markers alone and toward proven approaches built to assess total infection behavior.
This is the difference between identifying signals and delivering appropriate therapy.
Traditional Culture + AST
Guidance® TIRT Technology
| Culture + AST | PCR + AST | Total Infection Response Testing | |
|---|---|---|---|
| Clinical Question | Which organisms grow and how do they respond in vitro? | Which organisms or resistance markers are detected? | Which antibiotic demonstrates effectiveness against the infection as a whole? |
| Unit of Analysis | Individual cultured isolates | Detected organisms + associated markers | Total infection response — combined organism behavior |
| Polymicrobial Handling | Requires interpretation across multiple isolates | Requires interpretation across multiple detected targets | Inherently accounts for combined organism behavior |
| Basis for Insight | Inferred from lab growth conditions | Inferred from molecular detection + isolate susceptibility | Observed therapeutic response in patient-relevant conditions |
| Primary Limitation | Lab conditions may not reflect in vivo behavior | Genetic detection doesn't predict clinical response | — |
A Proven Path Forward.
Guidance UTI combines molecular detection with proprietary pooled phenotypic antibiotic susceptibility testing to evaluate how antibiotics perform against the infection as a whole, including polymicrobial infections. The result is faster, more actionable direction that helps clinicians make more confident first-pass decisions.
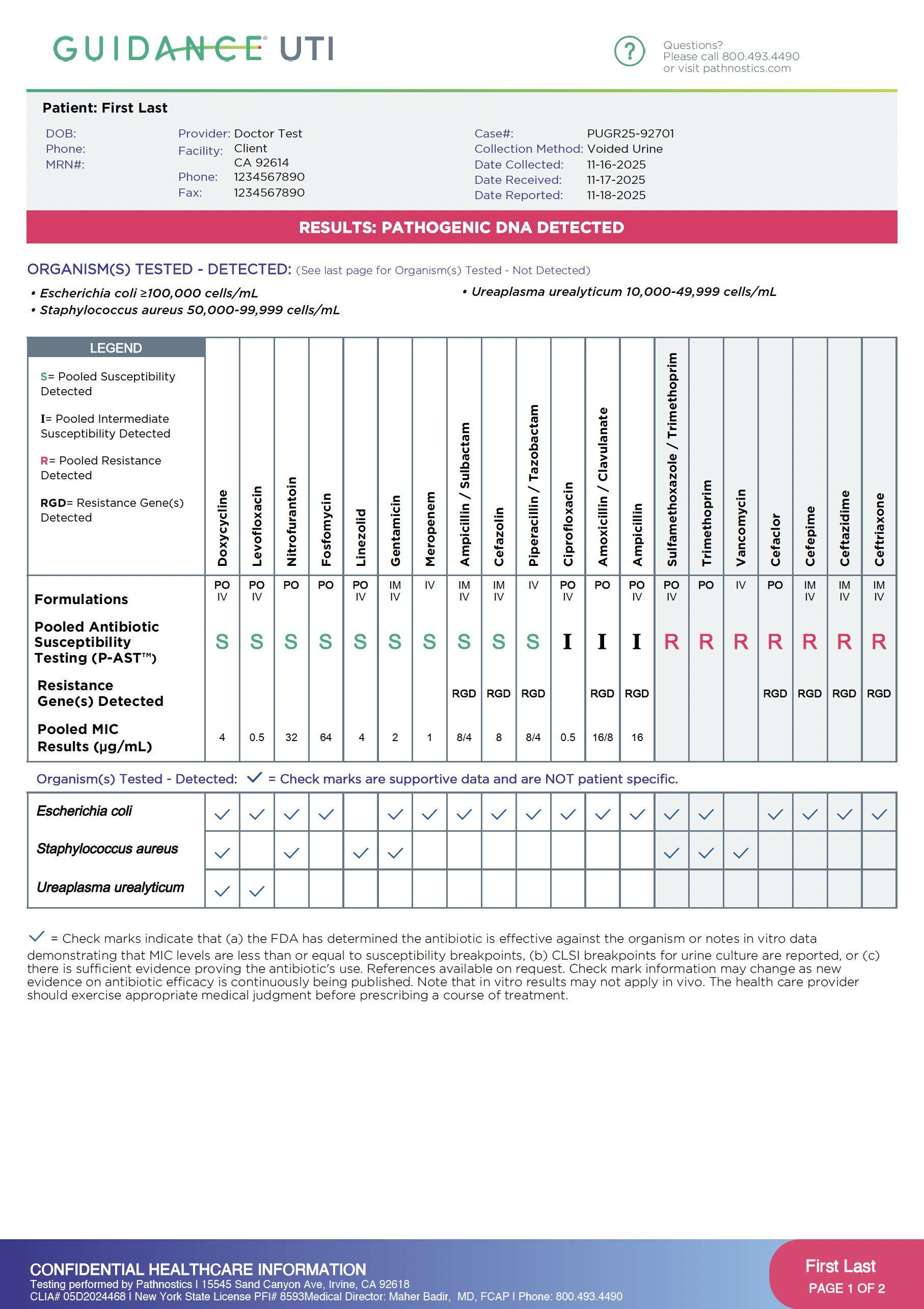
How Physicians Read a Guidance UTI Report
A short walkthrough of the P-AST report — what each section means and why it matters for treatment decisions.
Physician Perspectives.
"We've normalized retreatment in UTIs, and we shouldn't. Guidance is designed to be actionable — moving from detection to decision."
Infectious Disease
"Every retreatment increases antibiotic exposure and resistance pressure. Guidance helps clinicians choose targeted therapy sooner."
Pathnostics Provider
"The Guidance @Home program has extended our reach, ensuring hospital-grade diagnostics in a home setting."
Pathnostics Provider
Extend Better UTI Diagnostics Beyond the Four Walls of the Health System.
Not every patient can provide a sample in clinic or return easily for follow-up.
Guidance @Home extends the same diagnostic approach to patients wherever they are, helping practices protect continuity, preserve testing opportunities, and maintain access to higher-quality direction outside the four walls of the office.
Proof Matters in a Category
Full of Claims.
Pathnostics' differentiation is not a marketing story. It is a clinical and scientific one. Guidance UTI is supported by peer-reviewed publications, guideline recognition, and growing clinician adoption. In a market where many claims are easy to make, evidence is what earns trust.
We do not ask clinicians to believe a theory. We show them evidence.
Polymicrobial Antibiotic Susceptibility Testing in UTI Management
Clinical validation of P-AST methodology for polymicrobial urinary tract infections.
Download PDF →Treatment Interaction and Resistance Testing: A New Diagnostic Category
Defining the TIRT category and its clinical implications for antibiotic stewardship.
Download PDF →Retreatment Reduction Through Precision-Guided UTI Therapy
Evidence demonstrating reduced retreatment rates with Guidance UTI P-AST.
Download PDF →The Economic Impact of Diagnostic Failure in Outpatient UTI Care
Cost burden analysis of retreatment cycles and diagnostic inaccuracy.
Download PDF →Extending Precision Diagnostics to At-Home UTI Collection
Validation of at-home specimen collection for Total Infection Response Testing.
Download PDF →Reducing Unnecessary Antibiotic Exposure Through Targeted Diagnostics
How precision-guided therapy reduces broad-spectrum prescribing and resistance pressure.
Download PDF →Culture vs. P-AST: Head-to-Head Clinical Concordance Analysis
Side-by-side comparison of standard culture results and pooled susceptibility outcomes.
Download PDF →Pathnostics Evidence Cited in Updated AUA Clinical Guidelines
Summary of seven Pathnostics-published studies referenced in the 2024 AUA UTI guidelines update.
Download PDF →The Question Is Not Just What Is Detected.
It Is What Actually Works.
Guidance UTI helps clinicians move from trial-and-error toward better-informed first-pass therapy decisions.
Built for clinicians who want fewer avoidable repeats, better direction, and a more modern approach to UTI management.
- Coba et al. J Urol. 2019.
- Baunoch et al. Infect Drug Resist. 2021.
- Zhang et al. Front Microbiol. 2022.
- Harris et al. Microbiol Res. 2023.
- Price et al. J Clin Microbiol. 2016.
- Hansen et al. J Nurs Stud. 2022.
- Whelan et al. ASHE. 2022.
- Moreland et al. Front Cell Infect Microbiol. 2025.
- Daly et al. JOJ Uro Nephron. 2020.
- Vollstedt et al. J Surg Urol. 2020.
- Festa et al. Antibiotics. 2025.
- Haley et al. Diagnostics. 2023.